Unlocking the Spine
The Upper Complexity
This chapter begins to detail the application of technique. Methodology will scale in particularity; from specifics to each and every rib and vertebrae to more general soft-tissue, adaptable to most modalities in manual therapy.
In this section we are looking at common patterns and issues in the upper thoracic spine and ribcage.
...
To unlock and restore mobility to the spinal column and body requires a sequential and comprehensive effort. Our intent is to change the body more or less by considering its 'plumbing'. The plumbing we are most interested in is within the nervous system. To summarize previous sections; the neural system is a 'fluid' system which runs in-between bone (the "interosseous space") at the spine and rib cage. Distortions in those bony segments upset fluid dynamics in the neural system that runs between. Strategically, in a fluid system with blockages and compressions, it makes sense to work from the biggest blockages backwards. Otherwise we risk, by virtue of first opening and releasing the smaller blockages in a system, sending both pressure and demand into those larger blockages and causing strain at those points.
The Upper Complexity
This chapter begins to detail the application of technique. Methodology will scale in particularity; from specifics to each and every rib and vertebrae to more general soft-tissue, adaptable to most modalities in manual therapy.
In this section we are looking at common patterns and issues in the upper thoracic spine and ribcage.
...
To unlock and restore mobility to the spinal column and body requires a sequential and comprehensive effort. Our intent is to change the body more or less by considering its 'plumbing'. The plumbing we are most interested in is within the nervous system. To summarize previous sections; the neural system is a 'fluid' system which runs in-between bone (the "interosseous space") at the spine and rib cage. Distortions in those bony segments upset fluid dynamics in the neural system that runs between. Strategically, in a fluid system with blockages and compressions, it makes sense to work from the biggest blockages backwards. Otherwise we risk, by virtue of first opening and releasing the smaller blockages in a system, sending both pressure and demand into those larger blockages and causing strain at those points.
|
It is at the upper thoracic and shoulders in the human form that typically has the least interosseous space available and first begins to hold and fixate. These holdings translate into blockages and compressions into the fluid aspects of the neurological system, compromising the flow of cerebrospinal fluid (CSF). Fixations and distortions in the upper thoracic and shoulders in turn also hold distortion and patterns throughout the rest of the body. ... To unlock the twist we must begin where the twist is most locked. |

Interosseous (between-bone) space at the spine and rib cage.
|
Section A
The Basics - Where to start
In Theoretics 1 we covered the subject of innate tendencies towards distortion in the human form. Generally, the less interosseous space available, the more likely a movement fixation and ultimately a structural distortion will occur. Where interosseous space is typically lacking in the human body is in the thoracic - especially the upper thoracic and also notably, through the lateral aspects/sides of the body. Taken together, we find that the shoulder area has a number of structural vulnerabilities built-in. These innate tendencies and vulnerabilities create a strong likelihood that some of the larger and most important blockages and compressions in the neurological system will occur there.
A brief repeat of the end of Theoretics 1:
Ribs 1-5
Above Rib 6, the ribs become consecutively smaller, and with trauma, distortion, and the force of gravity over time, the smaller ribs above tend to tuck and lodge into the larger ribs below, creating distorted pressures on the vertebrae attached and behind. The overall effect is neural and spatial compression at the primarily, cardiovascular area of the body.
T1/Rib 1
Rib 1 not only displays a tendency to slip and lodge into the larger Rib 2 below, but also tends to get trapped behind the clavicle above. Compressive force and distorted pressure is transferred through the rib to the vertebrae (T1 and adjoining C7) and also to the vertebrae that are physically behind Rib 1: T3/T4.
The Basics - Where to start
In Theoretics 1 we covered the subject of innate tendencies towards distortion in the human form. Generally, the less interosseous space available, the more likely a movement fixation and ultimately a structural distortion will occur. Where interosseous space is typically lacking in the human body is in the thoracic - especially the upper thoracic and also notably, through the lateral aspects/sides of the body. Taken together, we find that the shoulder area has a number of structural vulnerabilities built-in. These innate tendencies and vulnerabilities create a strong likelihood that some of the larger and most important blockages and compressions in the neurological system will occur there.
A brief repeat of the end of Theoretics 1:
Ribs 1-5
Above Rib 6, the ribs become consecutively smaller, and with trauma, distortion, and the force of gravity over time, the smaller ribs above tend to tuck and lodge into the larger ribs below, creating distorted pressures on the vertebrae attached and behind. The overall effect is neural and spatial compression at the primarily, cardiovascular area of the body.
T1/Rib 1
Rib 1 not only displays a tendency to slip and lodge into the larger Rib 2 below, but also tends to get trapped behind the clavicle above. Compressive force and distorted pressure is transferred through the rib to the vertebrae (T1 and adjoining C7) and also to the vertebrae that are physically behind Rib 1: T3/T4.
|
Ribs 2, 3 & 4
These Ribs also share double tendencies towards distortion. Both Ribs display a tendency to fixate into the larger ribs below, however, the tendency is exacerbated by the shoulder girdle - acromion, scapula, and clavicle. The weight and spacial restrictions of the shoulder girdle heighten the tendencies for Ribs 2, 3, & 4 to fixate laterally - i.e.: in the armpit, under the shoulder as well as under the scapula. Cumulatively, we have a multitude of reasons to be quite suspicious of the entirety of the upper thoracic and shoulder girdle and many grounds to first focus our energies there. However, we still need to get more specific and answer the question: Where do we start? The Left Axis Here we reference back to Theoretics 2 to put that information to work for us. In the picture to the right, we again have a random sampling of past clients, most of which show a tendency for body mass in the upper thoracics to have shifted rightwards of a center line/axis going through their pelvis and legs. As body mass shifts to the right, the vertical axis itself relatively shifts to the left. I refer to this as the "Left Axis" and find that in the average human body, the vertical axis of orientation, rotation and structural distortion generally shifts leftward in the body. This means that as a human structure distorts, it is not necessarily distorting from a point of reference that is through the intended center of the body. This point of reference, of orientation, of balance in the human body, is itself distorted. As the human body shift rightwards of a left axis, the structure essentially "pinches" on the left side. As it does so, interosseous space, which is already in short supply in the shoulder girdle, is compromised and closes even more through the left side relative to the right. Hence, and bearing in mind that we want to work with the biggest blockages in the system, this tendency in structural distortion points us towards the left shoulder and left lateral thoracic as the smarter places to begin our interventions with manual therapy. It is here that interosseous space is generally compromised the most and first, relative to the rest of the body. Scoliosis Let's also take a look at some X-Rays, pictures, and depictions of the typical scoliosis pattern. We can also note where the spine in those instances tend to deviate from a center axis. We can definitely see a similar "Left Axis" orientation. But what else? Bear in mind that we've argued here that the scoliotic pattern is a compensatory pattern - essentially a way for the human body to distribute strain while staying upright in gravity. Scoliosis is a pattern which is arguably a general innate tendency in all human bodies as it distorts in the field of gravity. It is most easily recognizable when it occurs early in life (juvenile idiopathic scoliosis); when there is a great deal of interosseous space available through which the whole-body compensatory pattern may flourish. How does a scoliotic pattern occur? Commonly, a scoliosis not occurring after an identifiable trauma is called an "idiopathic" scoliosis - ("cause unknown"). While certainly a broad subject, many scoliotic patterns appear to wind their way up the spine, plausibly beginning with a twist in the coccyx and sacrum. I would again note that our species is the only mammal on the planet which regularly traumatizes the coccyx and sacrum area while learning to walk. Serious trauma at an early age to this area can cause a structural twist at the coccyx, sacrum and pelvis that would likely result in the compensatory pattern freely working its way up the spine with plentiful interosseous space in which to do so. The pattern would ultimately fixate in the shoulders, locking the distortion below. In an older, less-spacious body, the scoliotic pattern is also commonly seen, although it is often much more difficult to perceive - loss of space and decades of traumas (major and minor) can cloud the already clouded picture. With interosseous spacial restrictions gradually increasing with age, compensatory demand to structural distortion becomes that much harder to meet. Strain abounds, movement ceases and the structure is able to absorb less and less demands for change over time. Hence the lack of space assures that the older structure will not change in the same way or to the same degree as the younger scoliosis. However, the same patterns, the same forces, the same innate tendencies to the human makeup are equally as present. Scoliosis effects millions upon millions of people, in differing degrees and severities - from mild to debilitating. It is a common thing. In fact, spinal distortion itself, and acutely in the aged, is the norm. ... |

The random average body typically leans right respective of a center axis. Relatively, we can think of the center vertical axis as having shifted to the Left.

Typical scoliotic patterns. Note the closing of rib space through the left sides.

Spinal distortion is normal and gets more common with age.
|




|
The Importance is in the Commonalities
Given the typical scoliotic pattern taken in conjunction with the 'normal' deviation from a center vertical line seen in the 'normal' body, we can note two commonalities that tend to occur to the human spine and in particular to the upper thoracic and shoulder girdle. Both are rightwards shifts. With a scoliosis, we almost always see a strong, noticeable rightwards lateral shift at the thoracic level. In the average body, we also commonly note a rightwards shift to a center-line (the Left Axis). Thus, in a very large chunk of the human population, arguably the majority, we are seeing the same tendencies occurring in the thoracic and especially the upper thoracic. Are these two commonalities linked? Well, it is unlikely that the scoliotic tendencies we see are purely coincidental to the general tendencies seen in the random, average body. It is much more likely that we are looking at a similar problem and patterns expressed quite differently over time. Regardless of connection however, we are also looking at huge swaths of the human population that have relatively more compression to the neurologic system through the left thoracic relative to the right. (See also, Theoretics 2, High pressures and asymmetrical stresses in the scoliotic disc: https://www.ncbi.nlm.nih.gov/pubmed/17319969) Again we are chiefly concerned not with what is different in the human body across the species, but what is the same. And until we understand what is normal, we will never truly grasp what is different. Our strength of inquiry lies in the commonalities. From here we will begin to marry understanding and basic assessment into technique and practical application. |

The typical scoliosis often sees a strong rightwards lateral deviation in the thoracic.

Here a nude model, otherwise a picture of perfection to the public eye, shows a rightwards shift in the upper thoracic that appears most prominent at T3.
|
Section B
Technique
In regards to technique - unwinding is a very gentle, powerful way to work with the body and its tissues (See Practical 1) and our choice for technique. However, other techniques, such as regular 'swedish' massage and myofascial work, can achieve the same tissue-softening effects. With any well-performed technique the result is pretty much the same - the tissue softens.
All tissue exists within fascial membranes, and in softening tissue such as muscle tissue, a practitioner is necessarily also softening the fascia that encapsulates it. The makeup of the tissue within that fascial membrane is highly fluid in nature. The body itself is approximatelely 60% water/fluid, and this percentage of fluid is fairly constant through the fascial membranes that we are working with.
As we soften fascial membranes we are also effecting change to the fluid within by means of altering the fluid pressures within those membranes.
Here we are targeting specific locations in the body in which to soften the tissue and alter fluid pressures. Our goal is to induce movement in bony segments by softening the adjoining fascial membranes and changing the fluid pressures within. As we soften a fascial membrane that adjoins a bony segment, it creates a tendency for the bony segment to move in that direction - towards the direction of the lower fluid and fascial pressure.
Working in the Holes
In Physics we can broadly state that "particles flow from areas of high pressure to areas of lower pressure." Here the 'particle', is the bone itself within the system of fascial membranes. Thus, we essentially release and soften tissue in the direction of where we want things to go. This has us generally working in the "holes" of the body -- and, as we are discovering, one of the larger and
Technique
In regards to technique - unwinding is a very gentle, powerful way to work with the body and its tissues (See Practical 1) and our choice for technique. However, other techniques, such as regular 'swedish' massage and myofascial work, can achieve the same tissue-softening effects. With any well-performed technique the result is pretty much the same - the tissue softens.
All tissue exists within fascial membranes, and in softening tissue such as muscle tissue, a practitioner is necessarily also softening the fascia that encapsulates it. The makeup of the tissue within that fascial membrane is highly fluid in nature. The body itself is approximatelely 60% water/fluid, and this percentage of fluid is fairly constant through the fascial membranes that we are working with.
As we soften fascial membranes we are also effecting change to the fluid within by means of altering the fluid pressures within those membranes.
Here we are targeting specific locations in the body in which to soften the tissue and alter fluid pressures. Our goal is to induce movement in bony segments by softening the adjoining fascial membranes and changing the fluid pressures within. As we soften a fascial membrane that adjoins a bony segment, it creates a tendency for the bony segment to move in that direction - towards the direction of the lower fluid and fascial pressure.
Working in the Holes
In Physics we can broadly state that "particles flow from areas of high pressure to areas of lower pressure." Here the 'particle', is the bone itself within the system of fascial membranes. Thus, we essentially release and soften tissue in the direction of where we want things to go. This has us generally working in the "holes" of the body -- and, as we are discovering, one of the larger and
|
more general "holes" in the body, both in "normal" and scoliotic spines, often tends to be the left lateral thoracic - particularly, the left shoulder and left upper thoracic.
The "hole" is generally the concave aspect to a spinal curve. Below are some approximate starting points for structural interventions into the body that focus on the concave side of a lateral thoracic curvature. |

The Concave and Convex sides of a curve.
|

A starting point for manual interventions may often be here at the left shoulder and upper thoracic.
|

High into the left armpit and under the scapula, the ribs tend to fixate early, transferring strain to the vertebrae.
|
The idea behind these initial interventions is to first bring the spine closer to a lateral balance before addressing other distortions. To do so, we are first addressing the lateral aspects of ribcage and spine, versus the anterior and posterior (front and back) aspects of the ribcage. It is the lateral aspects - especially up into the shoulder, that tend to be the more lacking in interosseous space. Thus it is the lateral rib space that is most likely to close early on in the structural distortion process. These fixations impair movement throughout the entirety of the spine and hold other stubborn spinal patterns and distortions, including the more obvious anterior to posterior distortions such as kyphosis and lordosis.
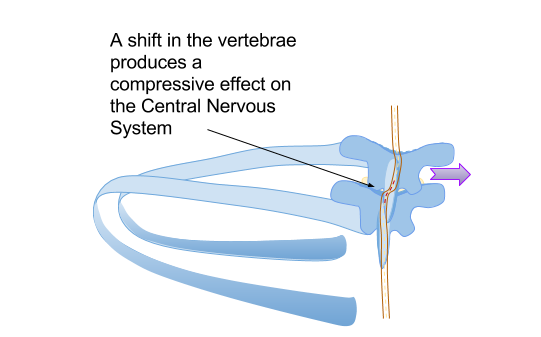
Problem Ribs & Spinal Shift
Fixations at the ribs are transferred directly to the vertebrae by virtue of a direct bony connection. If the rib is fixated left, it will tend to force the vertebrae towards a right lateral shift. As also explained in Theoretics 1, Section F, as a vertebrae shifts in the spinal column, it is the Central Nervous System (CNS) that largely feels the compression. Apart from an increase in neural compression, the lateral fixation of the rib will significantly reduce mobility throughout the whole of the rib as well as directly impact the movement of the vertebrae it is attached to. The repercussions will be felt through the entirety of the spinal column.
Problem Ribs & Spinal Shift
Fixations at the ribs are transferred directly to the vertebrae by virtue of a direct bony connection. If the rib is fixated left, it will tend to force the vertebrae towards a right lateral shift. As also explained in Theoretics 1, Section F, as a vertebrae shifts in the spinal column, it is the Central Nervous System (CNS) that largely feels the compression. Apart from an increase in neural compression, the lateral fixation of the rib will significantly reduce mobility throughout the whole of the rib as well as directly impact the movement of the vertebrae it is attached to. The repercussions will be felt through the entirety of the spinal column.


To ease these tendencies and restore movement and space to the rib and vertebrae, we must first address the lateral fixations present. As well, until some aspect of movement and space is restored through the lateral aspects, it will be exceedingly difficult to release other spinal restrictions in the body; notably, the vertebral and rib shifts that occur front to back (anterior to posterior) in the thoracic. The more lateral restrictions up into the armpit and under the scapula will act to hold the anterior to posterior restrictions while transmitting an element of strain through the entirety of the spine.
This may help to explain some of the historic difficulty in solving complex upper thoracic and shoulder issues, and as well -- the often temporary nature of structural interventions elsewhere in the body.
...
Danger, Will Robinson!
Taking a brief step away, in practical application, we must also look at the effects and issues encountered in opening tissue in the opposite manner. Broadly speaking, we might describe this as opening tissue where a "hump" occurs rather than a "hole". Intuitively, most bodyworkers just know it is unwise to take a wrecking ball, or a deep elbow, to a "hump" such as a kyphotic posterior thoracic curve (below). Such action will typically leave the client in an acutely painful state. In kyphosis, the tonus (tenseness) in the muscle and fascia of the hump is acting to brace the distortion and prevent the structure from falling into further distortion. But by releasing the holding patterns there, a practitioner may allow just that. Moreso, solely by virtue of softening the fascial membrane on top of the hump, the spinal column will be induced to move into a particular direction -- and in the case of the thoracic hump; further into distortion. As that occurs a chain of events will likely take place up and down the structure.
Below is a predictable scenario. Gravity is the acting force. The constant force downwards acts to compress the human structure and force distortion to occur outwards. In other words, it squishes us.
With a softening of the tissue here, a tendency is created for further posterior distortion of the structure at that location. Any further posterior distortion at the thoracic hump will also likely require the head to move forward to balance. As the process occurs, overall space is lost in the anterior chest along with a greater overall compression to both the cardiovascular (respiratory, circulatory) system, and the nervous system at that level.
Can bodywork do this? Yes...and it doesn't take much. If a bone moves a millimeter in the wrong direction, what is ultimately translated to the nervous system is quite a bit more when it comes to compression, especially to the Central Nervous System (CNS), which would feel the pinch in this scenario.
This may help to explain some of the historic difficulty in solving complex upper thoracic and shoulder issues, and as well -- the often temporary nature of structural interventions elsewhere in the body.
...
Danger, Will Robinson!
Taking a brief step away, in practical application, we must also look at the effects and issues encountered in opening tissue in the opposite manner. Broadly speaking, we might describe this as opening tissue where a "hump" occurs rather than a "hole". Intuitively, most bodyworkers just know it is unwise to take a wrecking ball, or a deep elbow, to a "hump" such as a kyphotic posterior thoracic curve (below). Such action will typically leave the client in an acutely painful state. In kyphosis, the tonus (tenseness) in the muscle and fascia of the hump is acting to brace the distortion and prevent the structure from falling into further distortion. But by releasing the holding patterns there, a practitioner may allow just that. Moreso, solely by virtue of softening the fascial membrane on top of the hump, the spinal column will be induced to move into a particular direction -- and in the case of the thoracic hump; further into distortion. As that occurs a chain of events will likely take place up and down the structure.
Below is a predictable scenario. Gravity is the acting force. The constant force downwards acts to compress the human structure and force distortion to occur outwards. In other words, it squishes us.
With a softening of the tissue here, a tendency is created for further posterior distortion of the structure at that location. Any further posterior distortion at the thoracic hump will also likely require the head to move forward to balance. As the process occurs, overall space is lost in the anterior chest along with a greater overall compression to both the cardiovascular (respiratory, circulatory) system, and the nervous system at that level.
Can bodywork do this? Yes...and it doesn't take much. If a bone moves a millimeter in the wrong direction, what is ultimately translated to the nervous system is quite a bit more when it comes to compression, especially to the Central Nervous System (CNS), which would feel the pinch in this scenario.

Softening tissue on the "hump" is generally problematic.
|

Spinal segments moving posteriorly will likely be balanced by segments moving anteriorly.
|
Holding patterns in the body are a two-sided coin. On one side they may prevent us from movement, balance and a sense of freedom; but on the other, they exist for a reason - often to prevent a structure from falling further into problem. Distortion, as noted, is more common then not. This brings us to a word not commonly heard in manual therapy - duty. Manual therapists, like other health professionals, have a duty to do no harm. When a spine is obviously at war with gravity and exhibits an overall embodiment of strain, there is a clear duty to the manual therapist to use the utmost caution.
|
All too often however this is lacking in manual therapy and especially in the world of massage, where the standard massage is 50 minutes face-down and 10 minutes face-up. The industry norms, bolstered by client expectations supported by glossy marketing, produce a decidedly unbalanced "therapy" in which the posterior aspects of the body receive the majority of the work.
The "prone" position, i.e. face-down in a head cradle, is generally a strained position for anyone with spinal distortion. Spinal distortion is again, the norm, especially over 50 years old. This equates to a staggeringly high percentage of the population experiencing discomfort from standard massage, simply by virtue of the positioning alone. The area where the thoracic "hump" so often occurs later in life, also happens to be the area of the posterior that is most accessible to the average, well-intentioned massage therapist. It is thus generally the posterior thoracic which receives a great portion of the work done; the posterior fascial membranes are softened, while significantly less attention is paid to to the anterior or lateral aspects of the body. By virtue of imbalanced work focused in the wrong place, this "standard" massage may compel a negative structural change over time, although it is the 'deep' tissue brand of massage that poses the heightened and more immediate dangers.
... Lateral Deviation We can now take the same understanding as applied to structural distortion occurring anterior to posterior (above) and apply it to spinal deviations that are more lateral in nature. In either case the structure and spine is in strain; movement is limited and the structure braces to remain erect in the field of gravity. Where, in the kyphosis example above, we were concerned that releasing holding patterns that would allow the body to fall further into anterior to posterior distortion, here we are concerned that releasing the incorrect tissue will allow the body to fall further into a lateral distortion. Again, because interosseous space is relatively more limited through the lateral aspects of the body, the neural space there is likely to be relatively more squeezed. Hence, in terms of sequencing our interventions into the body, the focus early on should be quite a bit into the sides of the body, especially above rib 6, where the ribs begin to get consecutively smaller and the risk of fixation into a rib below becomes heightened. On the average body, these lateral deviations are often hard to see. Typically, it will be the anterior to posterior distortion that catches our eye and our attentions. But it is the more hidden lateral distortion that may compress and effect the neural system to a greater degree and of which should take priority in the sequencing of our interventions. And again, these lateral deviations, distortions and fixations will impair movement through the entirety of the spine. Left unattended, they will derail any attempts to change other problems of the spine. ... Taken broadly, a manual therapy practitioner may be well-advised to prioritize work in the lateral holes and shallows of the body. Pay attention to the left side even though it may be the right side that is more symptomatic. Lateral Distortions will be addressed in greater detail in Methodology 2. Be advised, I am not trying to over-emphasize anything or any body part here, or just yet. The goal is comprehensive, whole-body change, which essentially requires attention everywhere. The intent is not for a practitioner to start spending half a session in the upper left thoracic. Indeed, as we shall see, we are first simply pressing for balanced work and the mere inclusion of the upper thoracic in standard manual therapy, particularly in the lateral aspects. ... |
    Standard massage often focuses on the thoracic 'hump'. This norm is strengthened by typical marketing - try a Google search of "massage" and then click on 'images'.

A high percentage of the population is uncomfortable during standard massage in the prone position.

Spinal distortion in the human body typically involves both anterior to posterior as well as lateral deviations.

Releasing tissue here may allow the body to fall further into a lateral distortion.
|
|
Practical Issues in Working With the Sides
We'll finish this section with a brief detour here to explore some of the practical realities in working with the lateral aspects of the body, i.e. the sides. In Rolfing/Rolf Structural Integration and it's various offshoots, a significant amount of time is dedicated to opening the sides of the body. The entire 3rd session of the ten-session Rolf 'recipe' is spent in the lateral aspects with attention all the way up into the armpit. Not surprisingly and congruent with our discussion here, the 3rd session of the Rolf recipe is typically regarded as the most profound session of the ten. While many other factors may contribute to the successes of Rolf/Rolfing Structural Integration, the mere attention to the sides of the body also appear to correlate. The use of the side-lying position also serves to differentiate the field from more standard manual therapy and mainstream massage. With massage particularly, the sides of the body typically receive very little attention, especially in proportion to other areas. Again, the typical massage consists of 50 minutes in a face-down position and 10 minutes face-up in a given hour. Side-lying, despite being the most comfortable and least vulnerable position available, is not regularly incorporated into standard massage -- due to the difficulties encountered in draping a naked body. It is, unfortunately, the widespread practice of receiving massage in the buff that helps drive the process. Naked massage is the norm, which then requires a specific draping of sheets and coverings. Draping is easy enough in supine or prone but in side-lying it is somewhat difficult and time-consuming for the therapist to do and slightly inconvenient to the client to get. For the average massage therapist, with a new client who has never experienced such a thing as side-lying and a diaper-drape, skipping the whole thing is ultimately the far more attractive option. This needs to change. |

Here I am demonstrating a side-lying Rolf Structural Integration technique. Rolf/Rolfing and its offshoots commonly employ the side-lying position and work extensively through the lateral aspects of the body.
    The industry norm. Side-lying work remains difficult and rare in standard massage because of the draping issues with naked clients.
|
Coming up next in Methodology 2:
Structures in Gravity
Explaining Structural Distortion and Pain
Body & Pattern Reading
Structures in Gravity
Explaining Structural Distortion and Pain
Body & Pattern Reading